Dr. Ward Dean answers your questions:
October 13th, 2022
As a world-renowned expert in anti-aging and longevity science, Dr. Dean is recognised for his pioneering work with nutritional and pharmacological approaches to delay aging and ameliorate age related diseases. Dr. Dean served as a member of the Gerontological Society of America, the American Geriatrics Society, the Association of Military Surgeons of the U.S., the American Physiological Society, and an Associate Fellow, Aerospace Medical Association and was also the first vice president of A4M.
Question 1
Dear Dr. Dean,
I have read a lot in your articles about metformin, and it seems to me to be very universal, having benefits for diabetes, weight loss, immunity, PCOS/ fertility and even cancer.
May I ask, why are its effects so broad? Is there a related factor between all these disorders?
I do appreciate all your knowledge.
Mrs. R.M., England
Answer
Dear Mrs. R.M.
Yes, there is a related factor that is shared by all the disorders you cited – it’s called the aging process.
I first learned about Metformin in 1981, when I read a book by a Russian physician/ scientist named Vladimir Dilman. 1 Dilman explained that Metformin was an antidiabetic drug that had several unique properties. He explained his belief that Metformin’s metabolic effects were due to a single mechanism—that of inhibiting fatty acid oxidation. He believed that diabetes resulted from impaired glucose tolerance, insulin resistance with secondary hyperinsulinemia, and enhanced gluconeogenesis by the liver – and he demonstrated that Metformin was able to reverse all these metabolic changes. He performed studies which showed that Metformin treatment increased the sensitivity of insulin receptors and that it also restored receptor sensitivity to all the body’s hormones – including those in the hypothalamus. In essence, Metformin seemed to be a “whole-body metabolic rejuvenator.”
Dilman was an anti-aging pioneer, who stated that “Metformin was the drug of choice for prevention of premature development of diseases of aging.” At that time, Dilman was a “voice in the wilderness”, as the only antidiabetic biguanide that had been available in the U.S. was phenformin, but it had been taken off the market in 1978 due to excess deaths caused by lactic acidosis. And Metformin, which had been available in Europe since the 1950s, was not approved for sale in the U.S. until the late 1990s.
Although Dilman had identified many of the metabolic effects of Metformin and credited it with its ability to prevent and treat hepatic steatosis (fatty liver), obesity, polycystic ovary syndrome (PCOS), diabetes mellitus, hypercholesterolemia, and atherosclerosis, and reduce the incidence of many cancers and other diseases of aging, the mechanisms causing these effects were not clearly identified, and they are still under investigation.
Several of Metformin’s “anti-aging mechanisms” were determined to be the inhibition of mitochondrial complex I in the electron transport chain (ETC) which resulted in the reduction of endogenous production of Reactive Oxygen Species (ROS—i.e., free radicals), and action as an activator of adenosine monophosphate kinase (AMPK) which results in the production of adenosine triphosphate (ATP), the universal energy molecule.
In 2012, Dr. Nir Barzilai, of the Albert Einstein College of Medicine in New York, clarified and enhanced metformin’s mechanisms, as illustrated in Fig. 1, 2, 3 As can be seen in the schematic, outside the cell (1, top) Metformin affects the receptor for cytokines, insulin, IGF-1, and adiponectin, all of which are activated with aging, and when modulated, are associated with longevity. Within the cell (2, middle) Metformin inhibits the inflammatory pathway, activates AMPK, inhibits mTOR, modulates oxidative stress, and removes senescent cells. These processes, together, (3, bottom) affect inflammation, cellular survival, stress defence, autophagy, and protein synthesis, which are all major biological outcomes associated with aging/longevity.
In 2013, an international research team proposed nine cellular and molecular Hallmarks of Aging that are generally considered to contribute to the aging process. namely: (1) Genomic Instability; (2) Epigenetic Alterations; (3) Loss of Proteostsis; (4) Deregulated Nutrient Sensing; (5) Mitochondrial Dysfunction; (6) Cellular Senescence; (7) Stem Cell Exhaustion; (8) Altered Intercellular Communication; and (9) Telomere Attrition. The impact this article had on the gerontological research community can be seen by the overwhelming response of scientists in the field by their proliferation of favorable citations, the number of which has increased every year since the article was published (Fig. 2). 4
Dr. Barzilai and his colleagues demonstrated how Metformin targets 4 of the hallmarks outlined in the Hallmarks of Aging article by looking at how it acts on AMPK, SIRT1, mTORC1, IIS pathways, inflammation, autophagy and macromolecular damage. These 4 inner circle hallmarks were:
- Deregulated Nutrient Sensing
- Loss of Proteostasis
- Genomic Instability
- Altered Intracellular Communication
The outer circle hallmarks outlined in the article are classed as secondary targets as their attenuation is mediated by Metformin’s role on a primary target (5)
Professor Dilman’s contributions to anti-aging medicine are profound. In addition to being an early proponent of the life-extending benefits of Metformin, members of his team such as Vladimir Anisimov and Vladimir Khavinson continue his research with Metformin and the anti-aging polypeptides of which Dilman was an early proponent and investigator.
I hope this somewhat technical answer responds to your question,
Respectfully,
Ward Dean, MD
Figures:
Figure 1. Metformin targets multiple pathways of Aging. See text for explanation. 2,3
This is figure 1, all that is required is the coloured circle.
Figure 2. Annual number of citations for the article, The Hallmarks of Aging, 4 since it was published in 2013, from PubMed. (2013-38; 2014-165; 2015-294; 2016-325; 2017-434; 2018-527; 2019-622; 2020-812; 2021-980; 2022-381 (so far)—Total-4245).
There is no graphic for figure 2, it is just this statement.
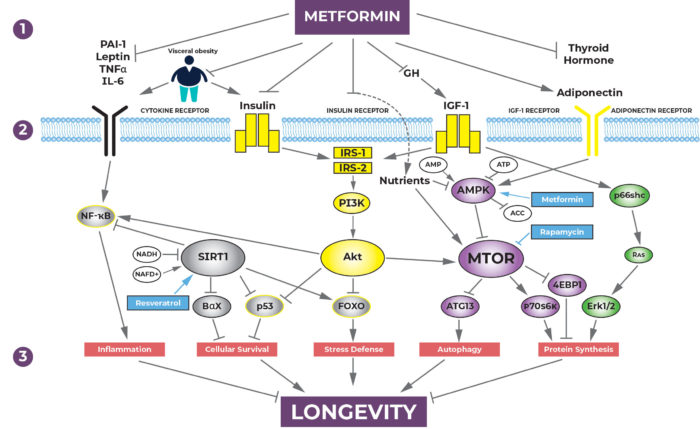
Figure 3. The primary and secondary targets of Metformin against the Hallmarks of Aging. 5 See text for explanation.
This is the rather complex schematic- we may have done this before- I will go back through some old issues, but I don’t know if you have on file? Note: There is a larger version of this that starts with ‘calorie restriction’ but the word METFORMIN needs to be placed into two boxes- as shown on the smaller version.
References:
- Dilman V. The Law of Deviation of Homeostasis and the Diseases of Aging, 1981, John Wright PSG, Inc. Boston.
- Barzilai N, Huffman DM, Muzumdar RH, and Bartke A. The Critical Role of Metabolic Pathways in Aging. Diabetes 61 1315-1322, 2012.
- Barzilai N, Crandall JP, Kritchevsky SB, and Espeland MA. Metformin as a Tool to Target Aging. Cell Metabolism 23, 1060-1065.
- Lopez-Otin C, Blasco MA, Partridge L, Serrano M, and Kroemer G (2013). The Hallmarks of Aging. Cell 153(6): 1194-1217. [PubMed: 23746838].
- Kukarni AS, Gubbi S, Barzilai N. Benefits of Metformin in Attenuating the Hallmarks of Aging. Cell Metab. 2020, July 07, doi.10.1016/j.cmet,2020.04.001.
Question 2
Dr Dr Dean
I would like to tell you about my issue and that I have been using liquid deprenyl on and off now, (more on than off) for 8 years at a dose of 2 or 3 mg daily. As a 78-year-old man I notice and like its effects. I feel more focused and mentally energised and have an arousal to my libido. Recently, I have developed a prostate issue of frequent urination, (particularly at night) and a slightly enlarged prostate- which naturally I do not want to get worse.
Please feel free to guide me on this and tell me if deprenyl is contraindicated.
With the greatest of respect.
Mr. H.M., Spain.
Answer
Dear HM,
If you’ve read my articles about Deprenyl in previous issues of Aging Matters™, you’re well-aware of its anti-aging, cognitive-enhancing effects. (1, 2) Deprenyl has few, if any, adverse effects, and I strongly doubt that it is adversely affecting your prostate.
It sounds like you have benign prostatic hyperplasia (BPH), which occurs in a high percentage of men as they get older. The standard medical treatment is to use 5-alpha reductase inhibitors like finasteride (Proscar®), which block the conversion of testosterone to dihydrotestosterone (DHT); alpha-receptor blockers like tamsulosin (Flo-Max®); and/or phosphodiesterase inhibitors (PDE-Is) like sildenafil (Viagra®). Some men respond better to one of the medications than others; often a combination works best.
A recent meta-analysis reviewed seven studies that compared regimens of combinations of tamsulosin and various PDE-Is. The authors concluded that for men with lower urinary tract symptoms (LUTS) due to BPH, the optimum regimen was daily tamsulosin (0.4 mg/day) plus sildenafil 25-50 mg 4 days per week. (3)
In addition to standard medical therapy (or instead of, as chosen by many men), there are likewise several over-the-counter substances that help to shrink the prostate and relieve urinary symptoms. These include saw palmetto extract (Seronoa repens, 320 mg/day); Pygeum Africanum (100-200 mg/day) (4); Stinging nettles (1200 mg/day) (5); and Beta sistosterol (60-195 mg/day). (6)
I hope those suggestions will do you as much good as the Deprenyl did.
Ward Dean, M.D.
References:
- Dean, W. Deprenyl and Alzheimer’s Disease update. Aging Matters, No. 3, 2016, 24-27
- Dean W, Deprenyl–an aphrodisiac & life extension agent. Aging Matters, Vol 3 No. 1, 2019, 11-17.
- Ma C, Zhang J, Cai Z, Xiong H, and Li H. Defining the efficacy and safety of Phosphodiesterase Type 5 Inhibitors with Tamsulosin for the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia with or without erectile dysfunction. BioMed Research International, 2020, Article ID 1419520, 8 pages.
- Stamatiou K, Magri V, Samara E, Perletti G. Serenoa repens and Pygeum Africanum in the treatment of BPH. Hellenic Urology, Vol 31, Issue 3, 2019, 33-40.
- Ghorbanibirgani A, Khalili A, Zamani L. The efficacy of stinging nettle (Urtica dioica) in patients with Benign Prostatic Hyperplasia: A randomized double-blind study in 100 patients. Iranian Red Crescent Medical Journal, Vol 13, No. 1, 2013, 9-10.
- Wilt TJ, Ishani A, MacDonald R, Stark G, Mulrow CD, Lau J. Beta sitosterols for benign prostatic hyperplasia (Review). Cochrane Database of Systematic Reviews, 2011, 1-20.
Question 3
Dear Dr. Dean,
I am about to start on a regular program of piracetam at 800 mg three times a day. After reading your books and online pieces I thought this was a good place to start.
My goal is to improve my awareness and creativity. My financial job is quite demanding, and I notice that I am not as ‘mentally bright’ as I was 10-years ago, (I am now 46) and I would like to stay ‘on top of my game’. So, can I ask you, is my dosage good and should I be considering anything else that is safe and effective in combination?
In gratitude.
Mr. W.V., Switzerland
Answer
Dear W.V.,
2,400 mg of Piracetam is a good starting dose to evaluate your tolerance (although adverse effects are very rare), but I usually recommend a higher dose. Most of the clinical studies of Piracetam used 4,800 mg—and many used even higher doses, ranging up to 12 gm (12,000 mg) per day!
Combining Piracetam with other cognitive enhancers that act by different mechanisms is a good idea – and may enable you to benefit from lower doses of each.
For example, Hydergine® (HyPro™) is a cerebral vasodilator, which improves blood flow to the brain, and with long-term use increases the growth of dendrites (neural connections) in the brain.
Modafinil (ModaPro™) and/or Adrafinil (AdraPro™) increase receptor sensitivity of a variety of cerebral neurotransmitters, and act as increasers of wakefulness and alertness. This class of medications is approved for those who suffer from “shift work sleep disorder,” but helps “wake up the brains” of the rest of us, without causing the adverse effects of stimulants like amphetamines.
For those who do not suffer from Parkinson’s or Alzheimer’s Disease, low doses (1-2 mg/day) of Selegeline (Deprenyl/ DepPro™) reduce the levels of Monoamine Oxidase B which tend to rise with age, enhancing cognitive performance, increasing libido, alleviating depression (and generally improving mood), and may increase the likelihood of living longer!
Centrophenoxine (Lucidril®, CentroPro™) acts as a mild cerebral stimulant and cell membrane stabilizer, that was developed by Prof. Imre Zs.-Nagy as a cognitive-enhancing anti-aging drug. The recommended dosage is 500 mg once or twice/day.
Over-the-counter supplements which may enhance cognitive performance include phosphatidylserine 300 mg/day, Acetyl-L-Carnitine 500 mg three times/day, and Ginkgo biloba.
Please let us know of your results,
Respectfully,
Ward Dean, MD
Question 4
Dear Dr. Dean,
My well-known doctor has recommended desmopressin to me; meanwhile, I have read that vasopressin is a natural version of it. I also see that they come in tablets or a nasal spray. Please give me your opinion of the two and their methods of application.
Thank you so much.
Miss M.G., California


Download the latest FREE AGING MATTERS MAGAZINE
V3 issue 42 2023

- Advertisement -