Attention Deficit Hyperactivity Disorder
November 28th, 2016Attention Deficit Hyperactivity Disorder
By Marios Kyriazis, M.D.
One of the most controversial syndromes of modern times is what we now call ‘Attention Deficit Hyperactivity Disorder’ (ADHD). This is a behavioural condition which has implications well beyond behaviour. As its name suggests, the condition includes being hyperactive, restless and fidgety, with a short attention span, as well being impulsive, anxious, a bad sleeper and experiencing ‘learning difficulties’. This last term is usually used only in a negative way, to imply that the patient cannot learn easily, whereas it should also imply that the patient is so special (positively or negatively), that her/his educational needs are also ‘special.’
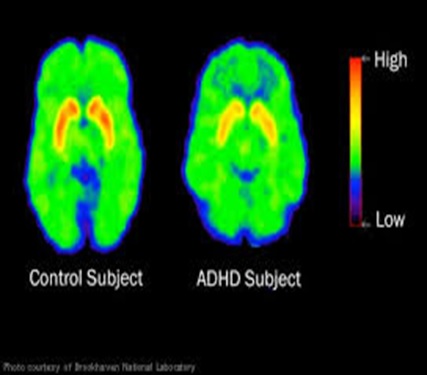
The difference between a normal brain, (left) and a patient with ADHD (right):
Image credit: Brookhaven National Laboratory
Usually, the condition is diagnosed when there is a significant change in the child’s life, such as starting school, or moving house. It is most common in children aged between 6 and 12 years but it can also persist in adult life. There is a 50% chance that a child born to a parent with ADHD will also have the condition. So, it is known that there is a genetic element.
Genetics
People with ADHD may have abnormalities of the DRD4 gene, (the dopamine receptor D4) which encodes the DRD4 receptor and it is found on chromosome 11. This particular receptor has been linked to conditions such as schizophrenia and Parkinson’s disease, as well as behavioural conditions. The DRD4 gene exhibits several polymorphisms (variations) which account for different functions. What is important here is that the gene has also been linked to ‘novelty seeking’ behaviour, i.e. a condition where the carrier constantly tries to experience new and unusual situations. This can be both a blessing and a curse, as it can be distressing but also helpful in expanding one’s horizons and worldview.
The connection of ADHD with the DRD4 gene also means that the condition could be treated by targeting this gene. There are some experimental and clinical drugs aiming to rebalance the function of the gene, and these include the anti-psychotic Clozapine, the anxiolytic Buspirone as well as apomorphine and Fananserin.
Despite the name, the DRD4 gene does not imply that ADHD is only due to low or only due to high dopamine activity. Research is contradictory and it shows that ADHD can be correlated to either low or high dopamine. But what is clear is that there is dysregulation of dopamine (1).
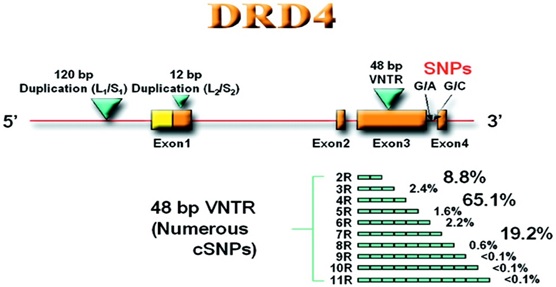
The human DRD4 gene, with its various components and interactions: Image credit: Yuan-Chun Ding et al. Evidence of positive selection acting at the human dopamine receptor D4 gene locus. PNAS 2002 99 (1) 309-314
***********************************************************************
A case study – perhaps with a profound significance (a six year old boy was diagnosed as having ADHD, because):
- He was hyperactive, with poor attention span at school.
- He was anxious and sometimes aggressive.
- His handwriting, as well as practical abilities were poor, (but he was good with computers).
- He was not interested in physical sport.
- Always in trouble due to his curiosity.
- He would prefer to eat sweets, chocolate and fatty foods, in contrast to his ‘normal’ younger sibling who preferred salads, fruit and lean meat.
A professional assessment concluded that the child was of exceptional intelligence and was acting badly only because of boredom and under-stimulation.
Speculation:
This child is an example of a new generation of humans who rely more on the cognitive and less on the physical. As we become more integrated with technology, Nature is preparing us accordingly: placing less emphasis on physical activities, and getting energy required for enhanced brain activity directly from ‘junk’ food.
Comment:
The example of the handwriting is striking: Why do we need to be able to handwrite in a society where everybody is using computers?
Conclusion:
What we now diagnose as a disease, could just be a normal feature of Nature, preparing humanity for the future!
It has to be said however that many ADHD sufferers and their families experience distress, sometimes considerable distress, due to the condition. So, irrespective of the question whether the condition is evolutionarily beneficial or not, it is necessary to attempt to treat at least some of the symptoms of ADHD. In this respect, there are several well-known drugs such as Adderall® and methylphenidate (Ritalin®) which stimulate dopamine and norepinephrine. Both drugs block reabsorption of dopamine and norepinephrine which means that these neurotransmitters remain active for longer.
Another group of pharmacological therapies include brain stimulants and nootropics such as:
- Centrophenoxine (meclofenoxane), which acts as a cognition enhancer, and is also an antioxidant (2).
- Adrafinil (the pro-drug of the stimulant modafinil) which improves cognition (3), and psychomotor function (4).
- the –‘racetams’ (for instance, aniracetam and piracetam), acting as stimulants (5), helping to improve speech problems (6), and improving behaviour, motor coordination and attention spans (7) confirmed in several studies (8,9).
In addition, two other drugs have also been found effective. These are selegiline and vasopressin.
Selegiline
Used in Parkinson’s disease, this monoamine oxidase inhibitor (MAOI) has also been shown to modulate the clinical symptoms of ADHD. It is important to note that no significant side effects have been reported. Selegiline is metabolized to amphetamine and methamphetamine both of which can be useful stimulants in the treatment of ADHD. Selegiline forms part of a host of treatments aiming to dampen down the clinical symptoms of ADHD (10).
The chemical structure of selegiline (deprenyl)
In a randomized, crossover, placebo-controlled study, (i.e. a formal and well-conducted study), researchers treated 11 children suffering from ADHD, aged 6-13 years. They found that that selegiline improves attention span, hyperactivity, learning, and interactions with other children (11), and concluded:
“Because the drug was not associated with negative side effects and did not specifically reduce symptoms of impulsivity, selegiline may be a preferred treatment for individuals who present with the primarily inattentive subtype of ADHD”.
In another study (12), 28 children were given either selegiline or methylphenidate (such as Ritalin®) and the two treatments were found of equal effectiveness, with the selegiline group reporting fewer side effects.
Vasopressin
Research shows that vasopressin may benefit children with attention deficit disorder (13). The arginine-vasopressin receptor (AVP) exhibits certain polymorphisms which have been linked to ADHD among others, therefore vasopressin treatment may be able to modulate this.
Vasopressin facilitates personal relations with respect to play-fighting and bonding (14). However, this needs specialist supervision, as issues with aggression may become a problem. It is typically used to treat nocturnal enuresis in ADHD patients (15). It is well known that children with ADHD show an increased prevalence of enuresis and other daytime voiding symptoms.
Conclusion
ADHD can cause distressing symptoms which can be relatively well-controlled through a combination of treatments. However, in my view, it should not carry the stigma of a mental or a behavioural disease. It may be a feature of natural evolutionary processes which have a tendency to improve humanity and get us ready for a full integration with technology.
References
- Badgaiyan RD, Sinha S, Sajjad M, Wack DS. Attenuated Tonic and Enhanced Phasic Release of Dopamine in Attention Deficit Hyperactivity Disorder. PLoS One. 2015 Sep 30;10(9):e0137326. doi: 10.1371/journal.pone.0137326. eCollection 2015
- Kovalev GI, Firstova IuIu, Salimov RM. Effects of piracetam and meclofenoxate on the brain NMDA and nicotinic receptors in mice with different exploratory efficacy in the cross maze test. Eksp Klin Farmakol. 2008 Jan-Feb;71(1):12-7
- Bagot KS, Kaminer Y. Efficacy of stimulants for cognitive enhancement in non-attention deficit hyperactivity disorder youth: a systematic review. Addiction. 2014 Apr;109(4):547-57
- Quisenberry AJ, Baker LE. Dopaminergic mediation of the discriminative stimulus functions of modafinil in rats. Psychopharmacology (Berl). 2015 Sep 15. [Epub ahead of print]
- Levinson HN. Dramatic favorable responses of children with learning disabilities or dyslexia and attention deficit disorder to antimotion sickness medications: four case reports. Percept Mot Skills. 1991 Dec;73(3 Pt 1):723-38
- Etchepareborda MC. Neurocognitive and pharmacological approach to specific learning disorders]. Rev Neurol. 1999 Feb;28 Suppl 2:S81-93
- Zavadenko NN, Suvorinova N. Therapeutic efficacy of nootropil different doses in attention deficit hyperactivity disorder. Zh Nevrol Psikhiatr Im S S Korsakova. 2004;104(3):32-7
- Zavadenko NN, Suvorinova N. Atomoxetine and piracetam in the treatment of attention deficit hyperactivity disorder in children. Zh Nevrol Psikhiatr Im S S Korsakova. 2008;108(7):43-7
- Froestl W, Pfeifer A, Muhs A. Cognitive enhancers (nootropics). Part 3: drugs interacting with targets other than receptors or enzymes. disease-modifying drugs. J Alzheimers Dis. 2013;34(1):1-114. doi: 10.3233/JAD-121729
- De Sousa A, Kalra G. Drug therapy of attention deficit hyperactivity disorder: current trends. Mens Sana Monogr. 2012 Jan;10(1):45-69. doi: 10.4103/0973-1229.87261
- Rubinstein S, Malone MA, Roberts W, Logan WJ. Placebo-controlled study examining effects of selegiline in children with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol. 2006 Aug;16(4):404-15
- Akhondzadeh S, Tavakolian R, Davari-Ashtiani R, Arabgol F, Amini H. Selegiline in the treatment of attention deficit hyperactivity disorder in children: a double blind and randomized trial. Prog Neuropsychopharmacol Biol Psychiatry. 2003 Aug;27(5):841-5
- Eisenberg J, Chazan-Gologorsky S, Hattab J, Belmaker RH. A controlled trial of vasopressin treatment of childhood learning disorders. Biol Psychiatry. 1984 Jul;19(7):1137-41
- Cheng SY, Delville Y. Vasopressin facilitates play fighting in juvenile golden hamsters. Physiol Behav. 2009 Aug 4;98(1-2):242-6. doi: 10.1016/j.physbeh.2009.04.019
- Chertin B1, Koulikov D, Abu-Arafeh W, Mor Y, Shenfeld OZ, Farkas A. Treatment of nocturnal enuresis in children with attention deficit hyperactivity disorder. J Urol. 2007 Oct;178(4 Pt 2):1744-7




Download the latest FREE AGING MATTERS MAGAZINE
V3 issue 42 2023

- Advertisement -