Alleviating the symptoms of an aging prostate
November 28th, 2016Alleviating the symptoms of an aging prostate
By Leslie J. Farer
Growing bald isn’t the only unwelcome sign of advancing years; for most men, aging also goes hand in hand with bothersome lower urinary tract symptoms: night time awakenings for trips to the bathroom, the sudden and frequent urge to urinate, painful urination, even erectile dysfunction.
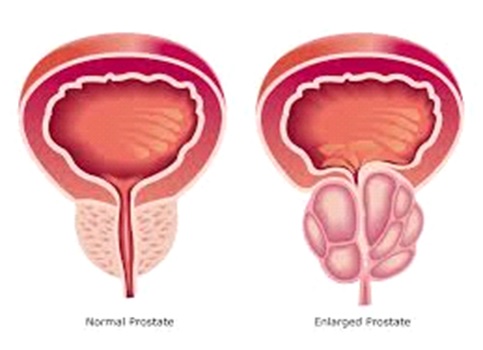
At the root of these issues may be the progressive enlargement of the prostate gland, which over time can grow from its original walnut-like size to reach the proportions of a lemon. Although prostate enlargement may be a sign of cancer, the most common cause is a non-malignant condition known as benign prostatic hyperplasia, which involves the growth of excess prostate tissue that eventually can obstruct the urinary tract, leading to impeded urine flow and troubling symptoms.
The good news is, through the use of phytotherapies (plant-derived treatments), nutraceuticals, dietary and lifestyle recommendations, and conventional drugs when necessary, the tissue-proliferating mechanisms that drive prostate enlargement can be attenuated, resulting in urinary symptom relief and improved quality of life for men over 40.
Age-related prostate growth and “LUTS”
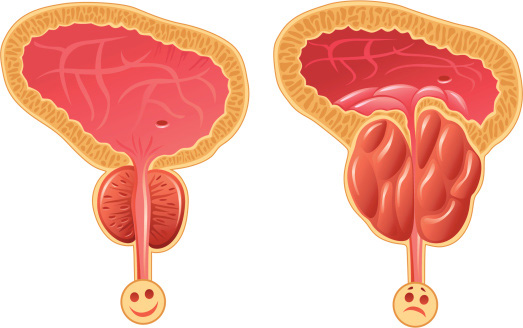
The prostate is a small gland of the male reproductive system that sits under the bladder and surrounds the urethra, the duct that carries urine from the bladder through the penis and out for excretion. Its main function is the production of seminal fluid. Over time, in most men, the prostate undergoes structural changes. By the time a man reaches his fifth decade, prostate cells can begin to multiply and pinch off the urethra, resulting in decreased urine flow. Even a small amount of growth can produce lower urinary tract symptoms (abbreviated “LUTS”), which include:
- urinary frequency and urgency
- weak urinary stream
- nighttime urination
- painful urination
- incomplete emptying of bladder
- sexual problems
The incidence of LUTS related to prostate enlargement is age-related, affecting approximately 50% of men age 60 to 90% of men age 85. (1) Obviously, safe and effective treatments are needed to counter this rising prevalence.
Ref.: health-headlines.org
Conditions related to prostate enlargement
The most common condition associated with a swollen prostate is benign prostatic hyperplasia (BPH). As the name implies, BPH involves the non-malignant (not associated with cancer) proliferation of cells in the prostate and formation of excess tissue, technically called “hyperplasia.” Besides annoying urinary symptoms, BPH can increase the risk of kidney damage and bladder infections; it can even lead to erectile dysfunction (ED). (2) A major factor in the development of hyperplasia, whether benign or malignant, is the influence of testosterone metabolites on the prostate, a hormone-sensitive organ.
One of these metabolites is dihydrotestosterone (DHT), converted from testosterone by the enzyme 5α-reductase. DHT is highly potent, and increased levels are associated with BPH and prostate cancer (3) (as well as hair loss, since 5α–reductase is also found in the scalp). Aging men also exhibit higher levels of another enzyme, aromatase, which converts testosterone into estrogen. (3) Like DHT, increased levels of estrogen promote cell proliferation. (3) Since BPH is an androgen- and estrogen-sensitive condition, an effective therapeutic strategy is to limit the activity of these enzymes (5α-reductase and aromatase), preventing the conversion of testosterone to hyperplasia-promoting DHT and estrogen. Below, we’ll see both drug and phytotherapies that target these enzymes.
Besides BPH, another non-malignant condition linked with prostate enlargement is prostatitis, which involves inflammation and/or infection of the prostate and shares many of the symptoms of BPH. Prostatitis can be chronic or acute, and is usually treated with anti-inflammatories or antibiotics. Prostate enlargement may also be a result of the malignant proliferation of tissue (i.e., prostate cancer). If you experience any urinary symptoms, see your health care provider as soon as possible to determine the cause, whether prostate enlargement (due to BPH, prostatitis, or prostate cancer), or a kidney problem or bladder infection. If prostate enlargement is detected, prostate cancer should be ruled out, but if diagnosed, must be treated with an individually-designed comprehensive medical and nutritional protocol as directed by your health care professional.
Note: This discussion focuses on the major non-malignant cause of prostate enlargement, BPH, although occasional reference will be made to prostate cancer prevention (since many of the natural and pharmacological agents outlined below have multiple mechanisms and benefits). A full discussion of prostate cancer is outside the scope of this article.
Treatment options for BPH/LUTS
The foundation that all men should establish to avoid the risk of, or ameliorate, prostate- related symptoms are a low fat, vegetable-rich whole foods diet and a healthy lifestyle. Meat and dairy products should be limited or eliminated, while generous servings of vegetables (including those high in carotenoids and Vitamin C) should be piled high on most plates. Additional nutritional support from supplemental zinc, selenium, vitamin C, lycopene, and essential fatty acids (EPA, DHA, and GLA) is also recommended, since all of these are beneficial in cases of BPH. Losing extra pounds, if necessary, maintaining an ideal body weight, controlling blood sugar, and exercising regularly will all lower the risk of BPH (and contribute to overall good health). These guidelines also apply to prostate cancer prevention (where cruciferous vegetables are particularly important in the diet, in addition to green tea, soy products, etc.).
On top of this foundation, the next level of support includes phytotherapies to alleviate symptoms in mild to moderate cases; in moderate to severe BPH/LUTS, drugs will likely be necessary. Peptide bioregulators may be beneficial in all cases, regardless of severity. Most men probably want to avoid surgery, especially in a sensitive part of the body, but surgical options do exist to either remove the prostate or reduce its size in order to relieve symptoms (although some readers might squirm to read this).
Conventional drugs for BPH
First, let’s look at standard pharmacological agents, of which there are several classes:
- 5-α-reductase inhibitors block the conversion of testosterone to DHT, helping to reduce the size of the prostate and ease symptoms, while preventing further growth. Finasteride (Proscar®) and dutasteride (Avodart®) are two FDA-approved 5α-reductase inhibitors that have been shown to improve urinary symptoms and reduce the risk of disease progression in BPH patients, (4,5) although they may cause some degree of sexual dysfunction. Both of these DHT-suppressing drugs have also been shown to reduce the risk of prostate cancer. (6,7)
- Aromatase inhibitors such as anastrozole (Arimidex®) have potential use in preventing the age-related increases in aromatase and estrogen that stimulate hyperplasia. (3) In men age 60 and older with low testosterone levels, one mg anastrozole daily increased testosterone and decreased estradiol production. (8) However, studies are few and further research is needed to confirm whether the estrogen-lowering capacity of aromatase inhibitors can significantly inhibit the prostate tissue over-proliferation that eventually leads to urinary symptoms.
- Phosphodiesterase-5 (PDE-5) inhibitors that are popular treatments for ED, such as tadalafil, (Cialis®), can also markedly improve LUTS in men with BPH. (9-11) (We saw earlier that BPH is a risk factor for ED and that the two conditions are related, so it follows that tadalafil can treat both.) Tadalafil is well tolerated with a favorable safety profile (10) and is approved worldwide for treating BPH-related urinary tract symptoms (whether or not they are accompanied by ED (11)).
- Desmopressin (Minirin®), another useful agent for BPH/LUTS, is particularly effective in reducing symptoms of nocturia (night time awakenings to urinate) that many men experience. Desmopressin is a synthetic analog of the natural antidiuretic hormone vasopressin, which plays a key role in regulating the body’s water balance, including promoting the reabsorption of water by the kidneys and reducing urine output. Vasopressin is approved as a drug for the treatment of diabetes insipidus and associated frequent urination, but its therapeutic use in nocturia is limited due to its short serum half-life. (12) Its analog desmopressin, on the other hand, with its longer activity in the bloodstream, (12) is more suitable for overnight use in limiting urination. (Note: Both vasopressin and desmopressin are also used off-label as potent memory and cognitive enhancers.) A review of 10 controlled trials on over 2,000 adults with nocturia found that desmopressin is effective in reducing the number of nighttime voids, and delaying the time to the first void. (13) A study specifically on men with LUTS/BPH and nocturia found that three months of desmopressin treatment cut the number of nocturnal voids by about half (from an average of 3.8 to 2), decreased urine volume, prolonged the number of hours of undisturbed sleep (due to fewer awakenings to void), and improved quality of life, with good tolerability. (14) (An interesting parallel study would have been to determine if the increased hours of sleep came with heightened memory of dreams, due to desmopressin’s cognitive-enhancing effects.) Desmopressin is used once daily before bedtime, starting with a low dose and increasing gradually until an effective dose is reached. Side effects are mild, but may include hyponatraemia (low serum sodium concentration) in patients age 65 years or older; serum sodium levels should be monitored while using desmopressin in these patients.
- Other drugs used to ease urinary symptoms include α1-adrenergic receptor blockers which increase urinary flow rate (though with sexual side effects) and antimuscarinics which relieve urinary urgency.
The above drugs are often used in combination. Although many of these are available through IAS, they should be used under the supervision of a physician. Note that certain of these conventional treatments for BPH (α1-adrenergic receptor blockers and 5α-reductase inhibitors) can cause sexual side effects, in addition to the ED that already accompanies many cases of BPH. Use of the natural remedies below combined with the lifestyle recommendations outlined earlier may decrease the need for, or lower the necessary dosage of, pharmacological agents, which will also result in a reduction of side effects.
Phytotherapies treat BPH safely and effectively
As a side effect-free alternative to drugs, numerous phytotherapies have been shown to successfully treat mild to moderate BPH/LUTS. Prostate Pro-2™ is a comprehensive formula containing four plant extracts that work synergistically to relieve troublesome urinary symptoms and promote overall prostate health, without unwanted side effects. Dozens of trials have been performed on the efficacy of these medicinal plants in treating BPH/LUTS, separately or in combination, and in comparison against conventional drugs.
- Urtica dioica (stinging nettle) root is a well-researched phytotherapy that acts by multiple pathways, including inhibition of aromatase in prostate tissue, (3) the same enzyme targeted by the drug anastrozole. In a placebo-controlled study on 558 patients with BPH/ LUTS, an impressive 81 percent of those who received Urtica for six months reported an improvement in symptoms (compared with 16 percent in the placebo group), and without side effects. (15) Other trials have demonstrated similar improvements, leading researchers to conclude that Urtica is a “safe therapeutic option for BPH, especially for reducing irritative symptoms and BPH-associated complications.” (16) Urtica also protects against prostate cancer by inhibiting proliferation of cancerous cells. (17)
- Pygeum africanum (African plum tree) bark extract has been used for decades in Europe and more recently in the USA to treat BPH/LUTS. Its active constituents include phytosterols (such as beta-sitosterol) that inhibit pro-inflammatory prostaglandins in prostate tissue. (18) Pygeum also suppresses 5α-reductase and aromatase, and when combined with Urtica, the enzyme-neutralizing effects are synergistic. (19) In one of the numerous studies on Pygeum, 50 mg of the extract twice daily for two months reduced nocturnal frequency of urination and increased urinary flow in BPH patients, side effect-free improvements that were maintained even one month after treatment. (20) A Cochrane Database review analyzing results of 18 randomized placebo-controlled trials on Pygeum involving a total of 1562 men with BPH concluded that the phytotherapy produced a “moderately large improvement” in overall urinary symptoms (including nighttime urination, urine flow, etc.) and that adverse effects were minimal and comparable to placebo. (21) In addition to its use in BPH/LUTS, Pygeum inhibits prostate cancer both in vitro and in vivo and is recommended for men at high risk for developing prostate cancer. (22,23)
- Seronoa repens or Sabal serrulata (Saw palmetto) berry extract has been treating prostate problems since the 1800’s, and today, it is probably the most widely used and well-known phytotherapy for BPH/LUTS. Saw palmetto contains several active compounds, including phytosterols, and has been shown to inhibit 5α-reductase (24) and reduce chronic inflammation of the prostate (25) which may contribute to BPH-related symptoms. Multiple trials have demonstrated its efficacy and safety, either singly, or combined with drugs or other phytotherapies. In the first clinical trial to evaluate the effect of saw palmetto on both BPH and sexual dysfunction, 320 mg of the extract daily for eight weeks cut urinary symptoms in half with a corresponding improvement in sexual performance. (2) Saw palmetto has been shown to be equally effective as some standard drugs, including finasteride or tamsulosin, (26) and when taken concurrently, it also augments their actions. A year-long study compared the efficacy and safety of saw palmetto plus tamsulosin (Flomax®, an α1-adrenergic receptor blocker) with tamsulosin alone and found that the combination treatment was more effective in improving LUTS, especially what the authors refer to as “storage symptoms,” (i.e., urinary urgency, frequency, and nocturia) than tamsulosin alone. (26) (About 20 percent of patients in each treatment group experienced adverse effects, however, due to tamsulosin.) Another trial compared a combination saw palmetto and Urtica extracts with finasteride. Both treatments produced equivalent improvements, but with more adverse events in the finasteride group than the phytotherapy group. (27) These studies underscore the safety and efficacy of saw palmetto, and its suitability for long-term use was demonstrated in an observational study on BPH patients taking 320 mg of the extract once daily for 10 years without disease progression or side effects. (28) In addition to BPH/LUTS and sexual dysfunction, saw palmetto may be helpful for chronic prostatitis (29), likely due to its anti-inflammatory action. It also exhibits chemopreventive properties. (29,30) (And, as a bonus, due to its DHT-inhibiting action, saw palmetto can potentially treat male pattern baldness! (31))
- Trifolium pratense (Red clover) is an emerging phytotherapy that may hold promise in treating BPH/LUTS and preventing prostate cancer. Studies show that isoflavone components in Trifolium can inhibit the proliferation of prostate cells, reduce their potential to become cancerous, and promote apoptosis (programmed cell death). (32,33)
To put it in a nutshell, these clinically proven phytotherapies act by different pathways to target the underlying mechanisms leading to prostate-related urinary symptoms (and even cancer). In a combination formula, such as Prostate Pro2™, their potencies are even further enhanced, making this an invaluable product to include in your regimen to improve and support prostate health.
The peptide bioregulator Libidon® rejuvenates the aging prostate
Now let’s discuss the prostate peptide bioregulator Libidon®. A major innovation in longevity therapies over the past few decades, led by Russian scientist Vladimir Khavinson, was the development of peptide bioregulators − short chains of amino acids (peptides) isolated from various animal tissues and organs. When purified and administered therapeutically, these peptides act at the genetic level to regenerate age-damaged tissues and restore the function of a particular organ. For example, retinal peptides initiate the formation of retinal and pigment cells in patients with retinal degeneration, thymic peptides stimulate immunity, and pineal peptides induce the aging pineal gland to manufacture melatonin. The mechanism behind these rejuvenating effects is complex: each short-chain peptide interacts with a gene’s DNA, transferring information encoded in its amino acid sequence and stimulating a process called protein synthesis, the manufacture of proteins according to the encoded genetic information. By “switching” on genes to synthesize specific proteins, peptide bioregulators can recover the structure and function of tissues and organs undergoing age-related deterioration. IAS carries a full range of 21 of these bioregulators (for organs ranging from adrenals to thyroid), including Libidon® for the prostate.
Khavinson and his team at the St. Petersburg Institute of Bioregulation and Gerontology have performed extensive research on the broad range of peptide bioregulators, including Libidon®, which was evaluated for its effect on a variety of prostate diseases. Khavinson’s experiments specifically on BPH involved administering, both intramuscularly and orally, prostate peptide bioregulators similar to Libidon® to BPH patients, which resulted in full or partial restoration of the normal tissue structure of the gland in 21 out of 27 cases; (34) in other words, in the majority of patients, age-related changes in prostate tissue were partially and in some case completely corrected. As a result of their regenerative potential, Khavinson recommends prostate peptide bioregulators (i.e., Libidon®) for all cases of BPH, from mild to severe.
Putting it all together – your plan for prostate health
Troubling symptoms resulting from an enlarged prostate are increasingly common in aging men; fortunately, as we’ve just seen, they are not inevitable, thanks to a variety of natural treatments and, if necessary, drugs.
The first step in preventing or ameliorating symptoms is to establish the foundation of dietary strategies and life style recommendations that we covered previously, with additional support from targeted nutraceuticals (zinc, selenium, etc.).
Next, phytotherapies should be added to relieve symptoms in mild to moderate cases of BPH/LUTS; Prostate Pro2™, a synergistic blend of four clinically proven botanical extracts, is an ideal choice for this purpose.
The peptide bioregulator Libidon® that acts by a unique and independent mechanism can also be included as another natural therapy for further support. If additional relief is needed in more severe cases, work with your health care professional in incorporating one or more conventional drugs to your regimen.
As mentioned, the use of phytotherapies combined with drug treatments will not only enhance the potencies of all of the active substances (pharmacological and natural), but will lower the necessary dosage of drug, and result in fewer side effects. Obviously, symptom relief may take some experimentation on your part − the natural therapies may be sufficient alone (Prostate Pro2™, Libidon® or both), or, in the worst cases, it may require the addition of a conventional drug(s) to reach an acceptable level of improvement.
However, by following the recommended lifestyle and dietary guidelines as a foundation to which you add an individually-tailored combination of natural treatments (and drugs, if necessary), you can relieve bothersome symptoms, while improving your overall health and quality of life.
| List of abbreviations | |
| BPH | benign prostatic hyperplasia |
| ED | erectile dysfunction |
| LUTS | lower urinary tract symptoms |
| DHT | dihydrotestosterone |
| PDE-5 | phosphodiesterase-5 |
References
- Pagano E, Laudato M, Griffo M, Capasso R. Phytotherapy of benign prostatic hyperplasia. A minireview. Phytother Res. 2014 Jul;28(7):949-55.
- Suter A, Saller R, Riedi E, Heinrich M. Improving BPH symptoms and sexual dysfunctions with a saw palmetto preparation? Results from a pilot trial. Phytother Res. 2013 Feb;27(2):218-26.
- [No authors listed] Urtica dioica; Urtica urens (nettle). Monograph. Altern Med Rev. 2007 Sep;12(3):280-4.
- Pirozzi L, Sountoulides P, Castellan P, et al. Current Pharmacological Treatment for Male LUTS due to BPH: Dutasteride or Finasteride? Curr Drug Targets. 2015;16(11):1165-71.
- Oelke M, Martinelli E. Pharmacological treatment of benign prostatic hyperplasia. Urologe A. 2016 Jan;55(1):81-96.
- Chau CH, Price DK, Till C, et al. Finasteride concentrations and prostate cancer risk: results from the Prostate Cancer Prevention Trial. PLoS One. 2015 May 8;10(5):e0126672.
- Andriole GL, Bostwick DG, Brawley OW, et al; REDUCE Study Group. Effect of dutasteride on the risk of prostate cancer. N Engl J Med. 2010 Apr 1;362(13):1192-202.
- Burnett-Bowie SA, Roupenian KC, Dere ME, Lee H, Leder BZ. Effects of aromatase inhibition in hypogonadal older men: a randomized, double-blind, placebo-controlled trial. Clin Endocrinol (Oxf). 2009 Jan;70(1):116-23.
- Brousil P, Shabbir M, Zacharakis E, Sahai A. PDE-5 Inhibitors for BPH-Associated LUTS. Curr Drug Targets. 2015;16(11):1180-6.
- Yokoyama O, Igawa Y, Takeda M, Yamaguchi T, Murakami M, Viktrup L. Tadalafil for lower urinary tract symptoms secondary to benign prostatic hyperplasia: a review of clinical data in Asian men and an update on the mechanism of action. Ther Adv Urol. 2015 Oct;7(5):249-64.
- Zhang LT, Park JK. Are phosphodiesterase type 5 inhibitors effective for the management of lower urinary symptoms suggestive of benign prostatic hyperplasia? World J Nephrol. 2015 Feb 6;4(1):138-47.
- http://uroweb.org/wp-content/uploads/BPH-20101.pdf (Guidelines on Conservative Treatment of Non-neurogenic Male LUTS)
- Ebell MH, Radke T, Gardner J. A systematic review of the efficacy and safety of desmopressin for nocturia in adults. J Urol. 2014 Sep;192(3):829-35.
- Berges R, Höfner K, Gedamke M, Oelke M. Impact of desmopressin on nocturia due to nocturnal polyuria in men with lower urinary tract symptoms suggestive of benign prostatic hyperplasia (LUTS/BPH). World J Urol. 2014 Oct;32(5):1163-70.
- Safarinejad MR. Urtica dioica for treatment of benign prostatic hyperplasia: a prospective, randomized, double-blind, placebo-controlled, crossover study. J Herb Pharmacother. 2005;5(4):1-11.
- Schneider T, Rübben H. Stinging nettle root extract (Bazoton-uno) in long term treatment of benign prostatic syndrome (BPS). Results of a randomized, double-blind, placebo controlled multicenter study after 12 months. Urologe A. 2004 Mar;43(3):302-6.
- Konrad L, Müller HH, Lenz C, Laubinger H, Aumüller G, Lichius JJ. Antiproliferative effect on human prostate cancer cells by a stinging nettle root (Urtica dioica) extract. Planta Med. 2000 Feb;66(1):44-7.
- [No authors listed] Altern Med Rev. 2002 Feb;7(1):71-4. Pygeum africanum (Prunus africanus) (African plum tree). Monograph.
- Hartmann RW, Mark M, Soldati F. Inhibition of 5 α-reductase and aromatase by PHL-00801 (Prostatonin®), a combination of PY102 (Pygeum africanum) and UR102 (Urtica dioica) extracts. Phytomedicine. 1996 Sep;3(2):121-8.
- Breza J, Dzurny O, Borowka A, et al. Efficacy and acceptability of tadenan (Pygeum africanum extract) in the treatment of benign prostatic hyperplasia (BPH): a multicentre trial in central Europe. Curr Med Res Opin. 1998;14(3):127-39.
- Wilt T, Ishani A, Mac Donald R, Rutks I, Stark G. A. Pygeum africanum for benign prostatic hyperplasia. Cochrane Database Syst Rev. 2002;(1):CD001044.
- Shenouda NS, Sakla MS, Newton LG, et al. Phytosterol Pygeum africanum regulates prostate cancer in vitro and in vivo. Endocrine. 2007 Feb;31(1):72-81.
- Larré S, Camparo P, Comperat E, et al. Biological effect of human serum collected before and after oral intake of Pygeum africanum on various benign prostate cell cultures. Asian J Androl. 2012 May;14(3):499-504.
- Habib FK, Ross M, Ho CK, Lyons V, Chapman K. Serenoa repens (Permixon) inhibits the 5alpha-reductase activity of human prostate cancer cell lines without interfering with PSA expression. Int J Cancer. 2005 Mar 20;114(2):190-4.
- Latil A, Pétrissans MT, Rouquet J, Robert G, de la Taille A. Effects of hexanic extract of Serenoa repens (Permixon® 160 mg) on inflammation biomarkers in the treatment of lower urinary tract symptoms related to benign prostatic hyperplasia. Prostate. 2015 Dec;75(16):1857-67.
- Ryu YW, Lim SW, Kim JH, Ahn SH, Choi JD. Comparison of tamsulosin plus serenoa repens with tamsulosin in the treatment of benign prostatic hyperplasia in Korean men: 1-year randomized open label study. Urol Int. 2015;94(2):187-93.
- Sökeland J. Combined sabal and urtica extract compared with finasteride in men with benign prostatic hyperplasia: analysis of prostate volume and therapeutic outcome. BJU Int. 2000 Sep;86(4):439-42.
- Aliaev IuG, Vinarov AZ, Demidko IuL, Spivak LG. The results of the 10-year study of efficacy and safety of Serenoa repens extract in patients at risk of progression of benign prostatic hyperplasia. Urologiia. 2013 Jul-Aug;(4):32-6.
- Zhan XX, Shang XJ, Huang YF. Zhonghua. Application of saw palmetto fruit extract in the treatment of prostate diseases. Nan Ke Xue. 2015 Sep;21(9):841-6.
- Zhou T, Yang Y, Zhang H, et al. Serenoa Repens Induces Growth Arrest, Apoptosis and Inactivation of STAT3 Signaling in Human Glioma Cells. Technol Cancer Res Treat. 2015 Dec;14(6):729-36.
- Prager N, Bickett K, French N, Marcovici G. A randomized, double-blind, placebo-controlled trial to determine the effectiveness of botanically derived inhibitors of 5-alpha-reductase in the treatment of androgenetic alopecia. J Altern Complement Med. 2002 Apr;8(2):143-52.
- Chen MY, Yan SC, Yin CP, et al. Red clover isoflavones inhibit the proliferation and promote the apoptosis of benign prostatic hyperplasia stromal cells. Zhonghua Nan Ke Xue. 2010 Jan;16(1):34-9.
- Slater M, Brown D, Husband A. In the prostatic epithelium, dietary isoflavones from red clover significantly increase estrogen receptor beta and E-cadherin expression but decrease transforming growth factor beta1. Prostate Cancer Prostatic Dis. 2002;5(1):16-21.
- antiaging-systems.com/articles/364-influence-of-peptide-bioregulators-on-morphology-of-parenchymatous-organs


Download the latest FREE AGING MATTERS MAGAZINE
V3 issue 42 2023

- Advertisement -